
![]() Download this fact sheet as a PDF to save and print.
Download this fact sheet as a PDF to save and print.
References are located at the bottom of this page.
References
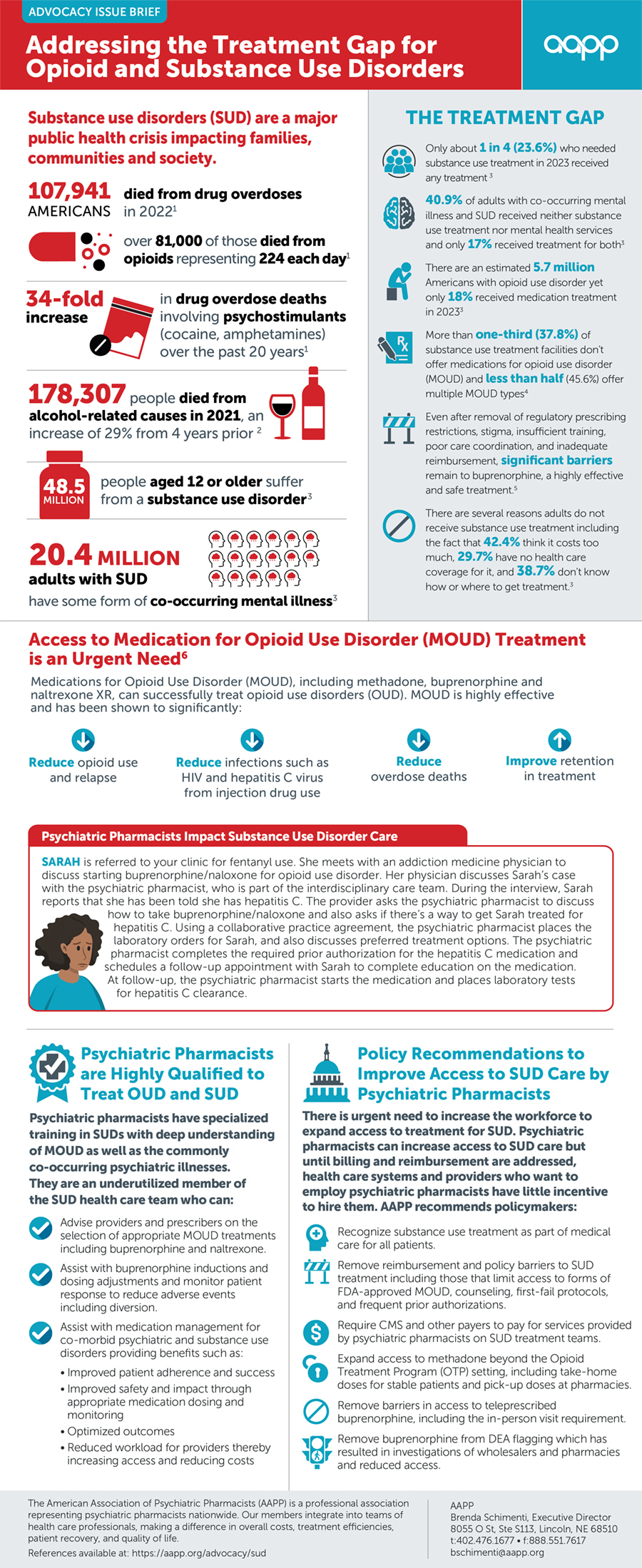
- Spencer MR, Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2002–2022. NCHS Data Brief, no 491. Hyattsville, MD: National Center for Health Statistics. 2024. DOI: https://dx.doi.org/10.15620/cdc:135849
- . Deaths from Excessive Alcohol Use — United States, 2016–2021. Mmwr Morb. Mortal. Wkly. Rep. 2024;73(8):154- 161. DOI: 10.15585/mmwr.mm7308a1. PubMed PMID: 38421934; PubMed Central PMCID: PMC10907037.
- Substance Abuse and Mental Health Services Administration. (2024). Key substance use and mental health indicators in the United States: Results from the 2023 National Survey on Drug Use and Health (HHS Publication No. PEP24-07-021, NSDUH Series H-59). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
- . Treatment Approaches for Opioid Use Disorder Offered in US Substance Use Treatment Facilities. JAMA. 2024;332(6):502. DOI: 10.1001/jama.2024.11913. PubMed PMID: 38990551.
- . Barriers and Facilitators to the Use of Medications for Opioid Use Disorder: a Rapid Review. J Gen Intern Med. 2020;35(S3):954- 963. DOI: 10.1007/s11606-020-06257-4. PubMed PMID: 33145687; PubMed Central PMCID: PMC7728943.
- Substance Abuse and Mental Health Services Administration. Medications for Opioid Use Disorder. Treatment Improvement Protocol (TIP) Series 63 Publication No. PEP21-02-01-002. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2021.